















The rush from methamphetamine lasts just a few minutes. The primary stimulant effects often stretch 6 to 12 hours, especially with higher doses and smoked or injected routes. After the high, a crash can last 1 to 3 days, followed by several days of low mood and sleep disruption. With repeated use or sleep deprivation, effects can extend longer. The average half-life of meth is around 10 hours, but varies widely by dose, route, and personal biology [1][2].
Methamphetamine doesn’t just hit fast, it lingers. For those using it, treating it, or trying to recover from it, knowing the actual timeline of meth’s effects can make a world of difference. This guide walks through each phase, from the initial rush to long-tail withdrawal, plus how treatment and support can reshape recovery.
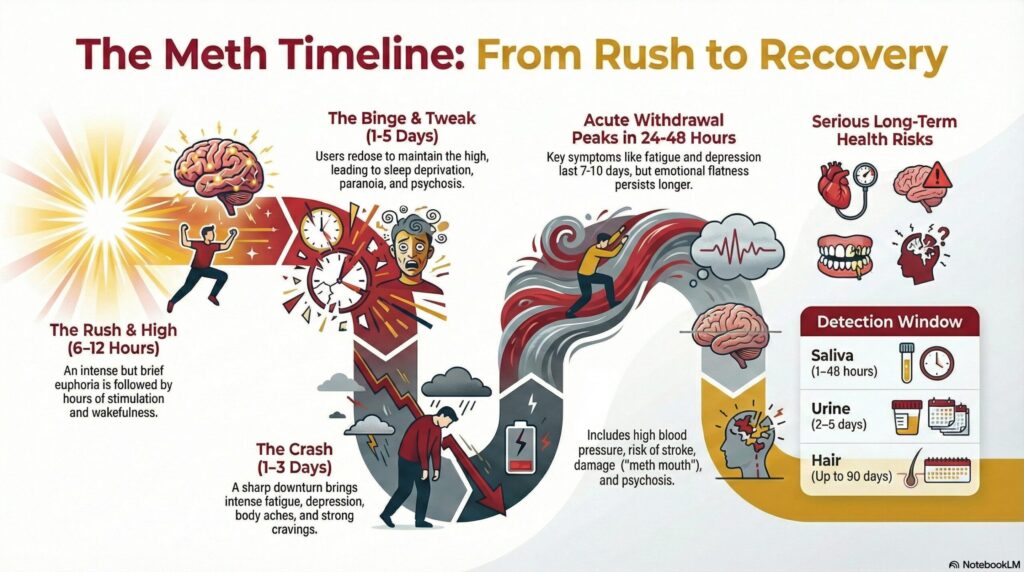
Meth Timeline at a Glance
The experience of meth happens in phases:
- Rush: Often under 30 minutes, brief, intense euphoria and physical surge
- High: Typically 6–12 hours of stimulation, energy, and alertness
- Crash: A sharp downturn lasting 1–3 days, with fatigue, depression, and cravings
- Normalization: Gradual return to baseline over 2–7 days, though mental fog or low motivation may linger
- Withdrawal Arc: Peak symptoms around 24 hours post-use, often resolving over 1–3 weeks [1][2][8]
Phase 1: The Rush (Lasts Minutes)
The rush is meth’s most intense moment, but it’s short. When smoked or injected, meth hits the brain in seconds, flooding dopamine systems. Users feel a wave of euphoria, sharpened focus, rapid heartbeat, and energy. This is often the part people chase, but it fades fast.
Most people redose to sustain this feeling. That’s where the danger of binging begins [1].
Phase 2: The High (6–12+ Hours)
The high that follows can last anywhere from 6 to 12 hours, longer for high doses or when smoked/injected. During this time:
- Appetite disappears
- Sleep feels impossible
- Speech and thoughts speed up
- Risk-taking and overconfidence rise
People may describe it as hyper-productive or laser-focused. But beneath that surface, physical and mental strain builds fast [2].
Phase 3: The Binge (1–5 Days for Some)
To maintain the high, some users enter binge cycles, dosing every few hours over multiple days. This is where dangerous patterns set in:
- Food and sleep vanish completely
- Paranoia, irritability, and impulsivity rise
- Tolerance grows rapidly, so effects fade even as risk climbs
By the end of a binge, the body and brain are deeply depleted, even though the person may still feel “wired” [1].
Phase 4: The Tweak (4–24 Hours)
Post-binge, users often hit a state known as tweaking. They may be exhausted but unable to sleep, agitated, and distrustful. It’s during this window that paranoia, auditory hallucinations, or psychosis may appear, especially in those with preexisting conditions or past trauma.
It’s a vulnerable time, both physically and psychologically, and can lead to risky behavior or conflict [1].
Phase 5: The Crash (1–3 Days)
After the rush, high, and tweak, the crash hits hard.
- Long periods of sleep (12–48 hours)
- Low mood or depression
- Intense hunger and thirst
- Body aches, headaches, and anxiety
Cravings can spike here, and some people redose just to escape the crash. This cycle makes quitting alone even harder [8].
Phase 6: The “Flat” Period (2–7 Days)
Even after sleep and nutrition return, people often describe a “flat” feeling, low motivation, emotional numbness, and scattered thinking. It’s not failure, it’s part of how the brain resets.
This “anhedonia” can last for several days or weeks, depending on prior use, sleep loss, and overall health [8].
Why the Timeline Varies
Several factors can stretch or shorten how long meth lasts:
- Route of use: Smoking or injecting hits fast and hard; snorting or swallowing builds more slowly
- Dose and purity: Stronger product = longer and harder stimulation
- Frequency of use: More use = more tolerance, shorter euphoria, longer crash
- Body chemistry: Liver and kidney function, body mass, hydration, and other health factors shift absorption
- Sleep and co-use: Sleep deprivation and combining substances (like alcohol or benzodiazepines) distort the timeline and risks [2][3]
Half-Life and Detection Windows of Meth
Meth’s average half-life is about 10 hours, though it ranges between 6 to 15 hours depending on urine pH and individual metabolism [2].
This means it can stay active in the system far longer than it “feels,” especially with redosing.
Typical Detection Windows:
| Test Type | Detection Window |
| Urine | 2–5 days (longer with heavy use) |
| Saliva | 1–48 hours |
| Blood | Several hours |
| Sweat patch | 7–14 days while worn |
| Hair | Up to 90 days |
Results vary by dose, hydration, frequency, and testing method [4].
What the Meth Crash and Withdrawal Feel Like
Meth withdrawal is mostly psychological—but that doesn’t make it easy.
Common Symptoms:
- Heavy fatigue
- Strong cravings
- Depression or hopelessness
- Irritability or anxiety
- Sleep disruption (too much or too little)
- Brain fog or difficulty concentrating
- Paranoia or, in some cases, psychosis
Time Course:
- Peak symptoms around 24–48 hours post-use
- Acute phase lasts 7–10 days
- “Flat” emotional period may continue for 2–4 weeks [8]
Why Meth Feels So Powerful And So Punishing After
Meth creates an overwhelming surge of dopamine and norepinephrine, key chemicals for reward and alertness. That’s why early use often feels like superhuman energy and confidence. But that same intensity disrupts natural brain signaling.
Over time, meth begins to reprogram your motivation, making everyday activities feel dull and unfulfilling without it. Sleep, food, and relationships lose priority. Cravings start to fire in response to stress or environmental cues. That’s why quitting isn’t just about willpower, it’s about resetting brain function and rebuilding routines [1].
Short- and Long-Term Health Risks of Meth Abuse
Meth use takes a toll, even in short periods. Risks grow with higher doses, repeated binges, and mixed substance use.
Key Health Harms:
- Cardiovascular: High blood pressure, arrhythmias, risk of stroke or heart attack, especially with heat or dehydration [1]
- Thermoregulation: Overheating can be life-threatening [1]
- Dental damage: Known as “meth mouth” from dry mouth, teeth grinding, and hygiene neglect [6]
- Infections: Skin abscesses, HIV or hepatitis C from shared syringes [1]
- Mental health: Anxiety, psychosis, paranoia, and trauma reactivation, especially after multi-day binges [1]
Harm Reduction Tips (Not a Replacement for Care)
For those who aren’t ready or able to quit, safety still matters. These strategies can reduce risk in the meantime:
- Avoid mixing with alcohol, benzos, or opioids, they increase overdose and dependence risk
- Hydrate and eat even small meals or snacks help regulate mood and body stress
- Cool overheated bodies shade, hydration, cool clothes; confusion or chest pain = emergency
- Use with others never alone, and with a plan if things go sideways
- Protect your mouth sugar-free gum, water, and avoiding sodas/sweets
- Sleep when you can even naps help; blackout curtains and quiet help restore balance
- Use clean gear, never share needles or cookers; syringe access programs can help
- Set a redose limit, like “no more after midnight” and ask a friend to hold you to it [1][6]
What Real Recovery Can Look Like
Medical Detox and Stabilization
For those in the tweak or crash phase, a safe environment helps stabilize mood, hydration, and sleep. Supervised detox may include short-term medications for sleep, agitation, or anxiety. Inpatient settings help monitor heart health and safety in high-risk windows [10].
Evidence-Based Treatments That Actually Work
- Contingency Management (CM): Offers real rewards for negative tests or treatment milestones, has some of the strongest results for meth and stimulant use [5]
- Cognitive Behavioral Therapy (CBT): Helps build new habits, manage triggers, and reduce reactivity [10]
- Integrated Care: Includes mental health treatment (depression, ADHD, trauma) and sleep support, key for long-term recovery [10]
Recovery Timeline: What to Expect
| Stage | What Happens |
| Week 1–2 | Crash symptoms peak, sleep returns, mood swings are common |
| Week 3–6 | Focus and energy improve, but pleasure may still feel “flat” at times |
| Months 2–6 | Mood evens out, motivation builds, brain chemistry stabilizes with routine care |
The brain and body often recover more than people expect, especially with sleep, structure, and social support [10].
When to Seek Emergency Care
Always seek help if you notice:
- Chest pain, rapid heartbeat, fainting
- Severe headache or confusion
- Overheating or high fever
- Hallucinations or paranoia with risk to self or others
- Seizure or suspected overdose [1]
Don’t wait. When in doubt, go to the ER or call for help.
Your Next Step Can Be Simple
You don’t need to have it all figured out. If you or someone you love is struggling with meth use, recovery starts with one move: a conversation.
Find Supportive, Evidence-Based Care at Red Rock Recovery
At Red Rock Recovery, we believe that healing is possible, without judgment or shame. Our programs combine medical detox, residential treatment, therapy, and sober living for a comprehensive path forward. Whether you need inpatient help or outpatient structure, we’ll help you navigate the next step.
Call now for a confidential assessment. Recovery starts with real support.
Sources
[1] National Institute on Drug Abuse. Methamphetamine. Bethesda (MD): U.S. Department of Health and Human Services; 2024. Available from: https://nida.nih.gov/research-topics/methamphetamine
[2] Cruickshank WJ, Dyer KR. A review of the clinical pharmacology of methamphetamine. Addiction. 2009;104(7):1085-1099. Available from: https://pubmed.ncbi.nlm.nih.gov/19426289/
[3] McIntyre IM, et al. Antemortem and Postmortem Methamphetamine Blood Concentrations. 2013. U.S. Department of Defense. Available from: https://media.defense.gov/2019/Sep/09/2002180420/-1/-1/0/CG%20069%20_V1%20ANTEMORTEM-POSTMORTEM%20METHAMPHETAMINE%20BLOOD%20CONCENTRATIONS.PDF
[4] Hadland SE, et al. Objective Testing—Urine and Other Drug Tests. Curr Probl Pediatr Adolesc Health Care. 2016. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4920965/
[5] Substance Abuse and Mental Health Services Administration. Using SAMHSA Funds to Implement Evidence-Based Contingency Management Services. 2025. Available from: https://www.samhsa.gov/resource/ebp/using-samhsa-funds-implement-evidence-based-contingency-management-services
[6] American Dental Association. Meth Mouth. ADA MouthHealthy. 2024. Available from: https://www.mouthhealthy.org/all-topics-a-z/meth-mouth
[7] MyHealth Alberta. Methamphetamine: What to Expect When Someone Quits. Alberta Health Services. Available from: https://myhealth.alberta.ca/alberta/Pages/Methamphetamine-what-to-expect-when-someone-quits.aspx
[8] American Dental Association. Methamphetamine (Oral-Health Topic). 2023. Available from: https://www.ada.org/resources/ada-library/oral-health-topics/methamphetamine
[9] NIDA. Mind Matters: The Body’s Response to Methamphetamine. 2019. Available from: https://nida.nih.gov/research-topics/parents-educators/mind-matter-series/methamphetamine
[10] SAMHSA. Treatment of Stimulant Use Disorders. 2020. Available from: https://library.samhsa.gov/sites/default/files/pep20-06-01-001.pdf